ContactUs
Rajiv Gandhi Cancer Institute and Research Centre
New Delhi - 110085
Rajiv Gandhi Cancer Institute and Research Centre
New Delhi - 110085
Presenting Complaints: Mr A, 49 Years Old Gentleman Presented To Us With Complaints Of Change In Voice For The Last 1 1/2 Months & Pain On Swallowing Food For The Last 3 Weeks. The Patient Is Accompanied By His Wife & Son & They Provided Additional History Of Noticing A Swelling On The Left Side Of His Neck For The Last 1 Month, Which has been Progressively Increasing In Size.
The patient was apparently well approximately 1 1/2 months back when he started noticing a change in his voice. He took symptomatic treatment but the change persisted. Approximately 2 weeks later, the relatives noted a swelling on the left side of the neck. Upon seeking medical attention from a GP, he was prescribed some antibiotics and told to return if symptoms persisted.
A week later the patient started noticing pain on swallowing, which was initially mild & intermittent (occurring especially with dry food). He returned to the GP & the patient was referred to an ENT Surgeon. The patient underwent a needle aspiration from the swelling in his neck & was referred to us for further evaluation and management.
Smoker - 25 pack years. 10-12 cigarette sticks/day. Occasional Alcohol intake.
No significant past medical or surgical history.
Upon clinical examination, patient's speech was noted to have a 'hot potato' quality. Average build with BMI - 25, height -, weight -, BSA -. His vitals were normal. His Karnofsky Performance Score was 90. No pallor/ icterus/ cyanosis/ clubbing/ pedal edema/ elevated JVP was noted.
He was noted to have a 3 x 2 cm lump on the left side of his neck just below the ramus of the mandible, with normal skin overlying it. It's surface appeared irregular and it's margins were difficult to distinguish from the surrounding structures. On palpating the lump, it was firm in consistency and non-tender with fixation to the underlying structures. It was non-cystic, non compressible, nonfluctuant & non-pulsatile (though transmitted pulsations from the carotid artery were felt). It was located just behind the sternocleidomastoid muscle at its cranial end (Level II). No other enlarged lymph node was noted in the ipsilateral or contra lateral neck.
No gross abnormality was noted on inspection & palpating of the oral cavity. Note was made of irregular nodularity on the base of tongue. On indirect laryngoscopy, a nodular growth was noted on the left base of tongue which was approaching the left vallecula inferiorly.
Biopsy revealed moderately differential squamous cell carcinoma. Staging work up on CT revealed a 3cm irregular contrast enhancing lesion in the left base of tongue and a 2.5 cm lymph node at level II of the neck. A PET-CT was done to evaluate presence of additional metastatic spread, which was negative.
The Radiotherapy process starts with the Radiation Oncologist discussing the need for radiotherapy with the patient & family under the following 5 headings, viz. Indication & Goal, Volume, Technique & Dose/ Time.
The simulation process consists of positioning the patient, creating a custom immobilization cast (to maintain the same position over all treatment days) & undergoing a high resolution contrast enhanced planning-CT scan.
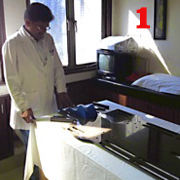
Simulation.
Figs 1 & 2: The positioning of the patient is done on a special board with markings to permit accurate & reproducible positioning subsequently. A neck rest is also placed to accurately reproduce the neck position. The patient is placed supine on the board, and aligned with the markings on the board. This is confirmed visually by aligning important surface landmarks, viz. the glabella, tip of the nose, sternal notch, umbilicus & pubic symphysis.
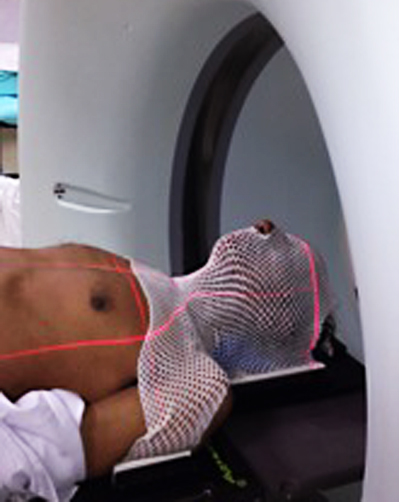
Fig 3: Once the patient is positioned, a custom thermoplastic cast is made. This helps in further reducing the variations which can arise from positioning the patient daily.
Figs 4 & 5: Once the cast is created, the patient is taken for planning-CT, where the patient is repositioned using the board & cast.
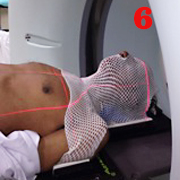
Fig 6: Tumor localization is aided by a laser guidance system which places a external reference point on the cast.
Treatment planning starts with a thorough evaluation of the planning CT by the radiation oncologist. Evaluation is focussed on correlating findings on clinical examination with radiological findings on the planning-CT. The aim is to ultimately create an accurate 3- Dimensional model of the patient, delineating the areas which are to be irradiated & important areas to be protected. (Figures 7 - 16)
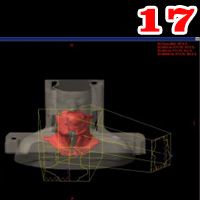
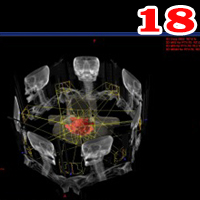
The medical physicist then analyzes this data and arranges multiple treatment beams with varying intensities to create a treatment plan. (Fig 17, 18)
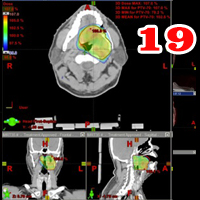
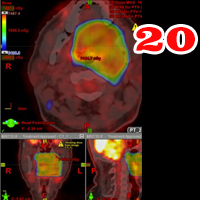
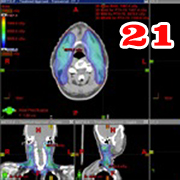
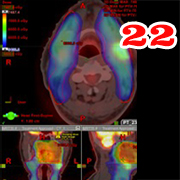
The treatment plan is then evaluated by the radiation oncologist (Figs 19 - 22) & approved for implementation.
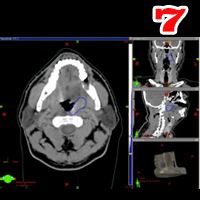
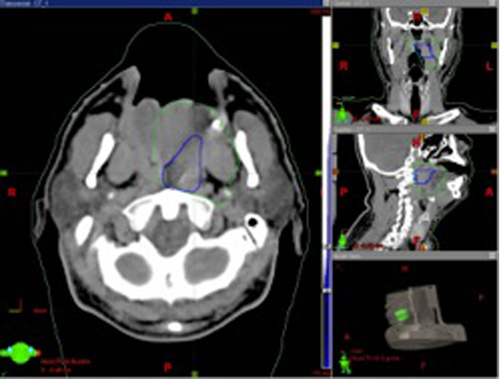
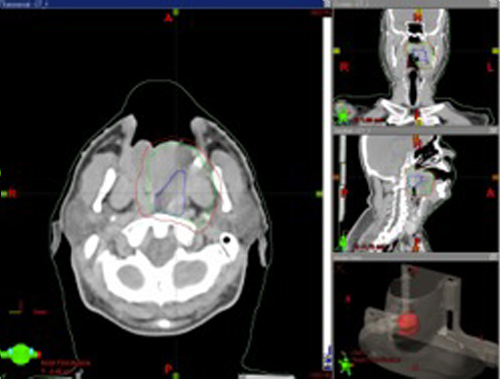
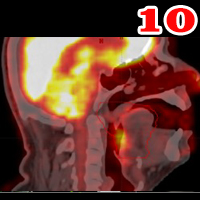
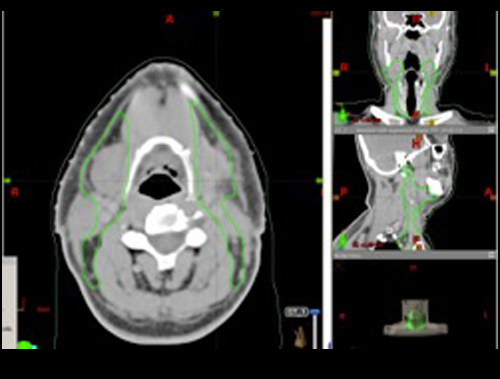
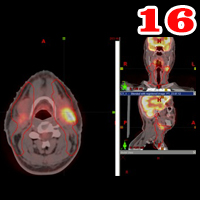
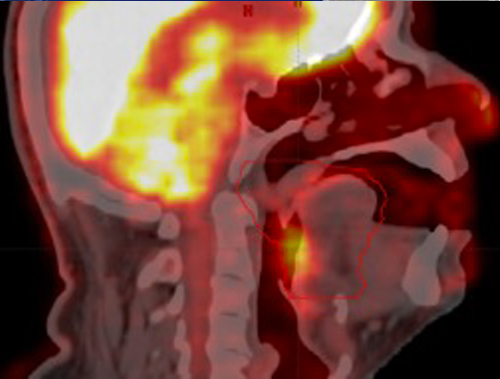
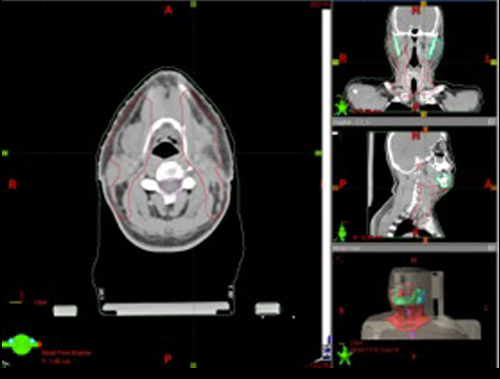
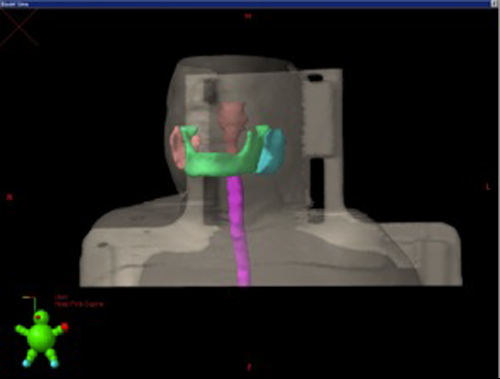
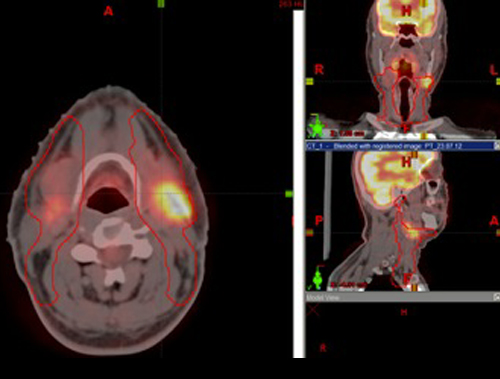
Treatment Planning. The following structures are contoured on the treatment planning system, Gross Tumor Volume* (Fig 7 - in Blue), Clinical Target Volume** (Fig 8 - in Green) & Planning Target Volume*** (Fig 9 - in Red). Fig 10: The treatment plan is also fused with the pretreatment PET-CT scan so as to aid in delineating the target volumes.
* Gross Tumor Volume - The visible tumor
* Clinical Target Volume - The area around the gross tumor which is likely to harbor microscopic disease.
Treatment Planning (continued).
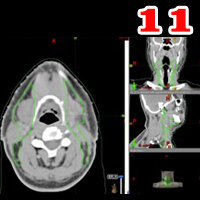
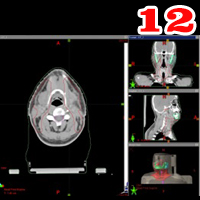
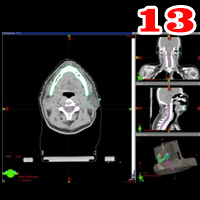
Figs 11 & 12: Since the neck also needs to be treated, the lymph node levels of the neck which may harbor disease are also delineated (Green). The neck is also given a PTV(Red). Fig 13: The organs which are to be protected are delineated next (Mandible - Dark Green. Parotid Glands - Blue & Orange. Spinal Canal - Pink. Brain stem - Brown).
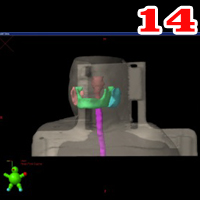
Fig 14: 3-Dimensional model of the patient showing the various organs which are to be protected.
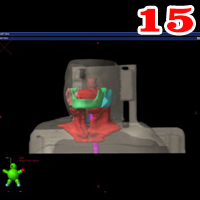
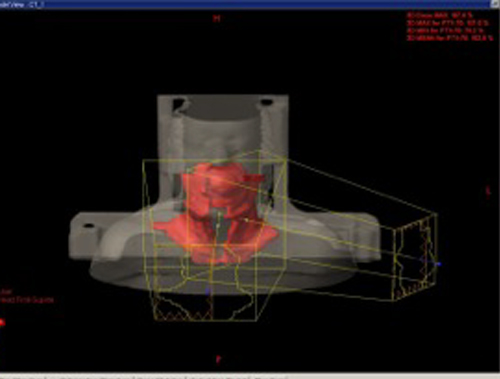
Fig 15: 3-Dimensional model of the patient with area to be treated (Red), in relation to the areas to be protected. Note the close proximity of both.
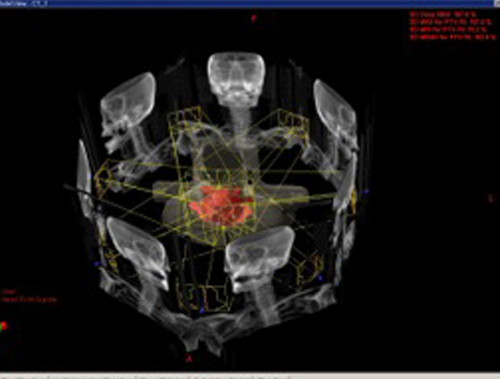
Figs 17 & 18: Generating an IMRT treatment plan.
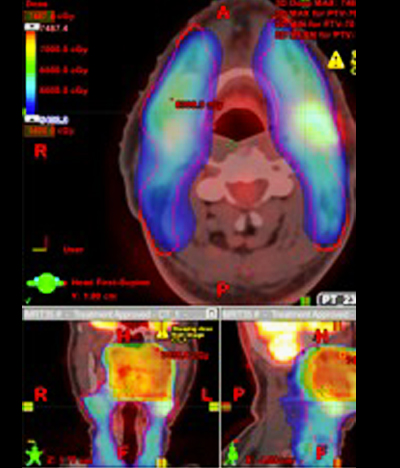
Figs 19 & 20: Dose color wash showing adequate coverage of the Primary tumor PTV & verified on PET.
Figs 21 & 22: Dose color wash showing adequate coverage of neck & verified on PET.
Once the plan is ready, it is ready to be implemented on the patient, usually after an interval of 2-3 days after undergoing simulation.
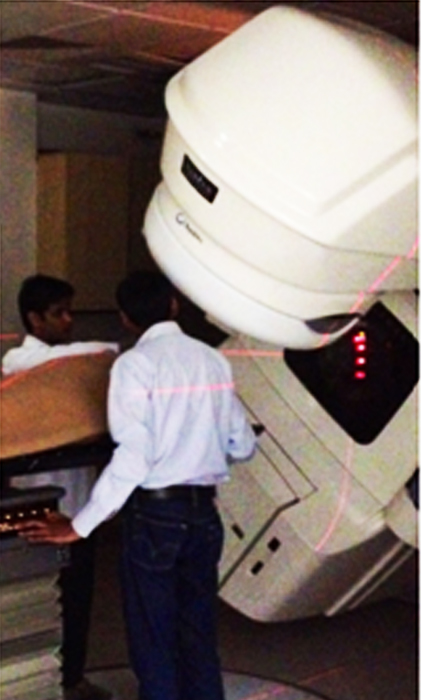
The process of plan implementation is a technically intensive process, as the data from the treatment planning system is transferred to the treatment machine (In this case, Varian Clinac 2100c RapidArc with a Cone beam CT [On Board Imager]) (Fig 23)
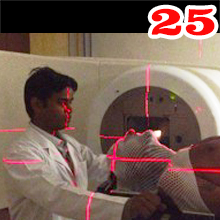
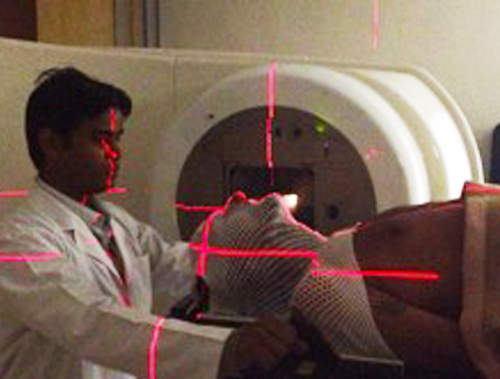
Implementation consists of setup & treatment delivery in the same position as simulation. The principles of setup remain the same as that of simulation (Fig 24). The laser guidance system on the machine (Fig 25) & on the CT Simulator (at the time of simulation, Fig 6) help in further verifying that the patient is accurately set up.
Prior to treatment delivery, verification CT scan is done on the treatment machine with the On Board Imager. The verification CT is then matched to the Planning CT to further increase the accuracy of treatment delivery.
Once the plan is accurately matched, the first treatment fraction is delivered. Subsequently, when the patient arrives for further fractions, the time required to deliver the treatment is reduced significantly.
During the course of treatment, patients are reviewed weekly by the radiation oncologist & blood tests done.
Precautions concerning skin care, oral hygiene & nutrition which the patient needs to follow are also explained to the patient.
Implementation.
Fig 23: Varian Clinac 2100c RapidArc with Cone Beam CT (On Board Imager).
Fig 24: Patient being set up on treatment machine.
Figs 25 - 27: Patient's position is confirmed using the laser guidance system, following which patient is ready for receiving the first fraction of Radiotherapy.
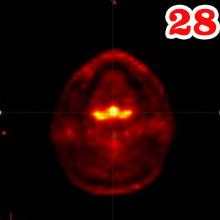
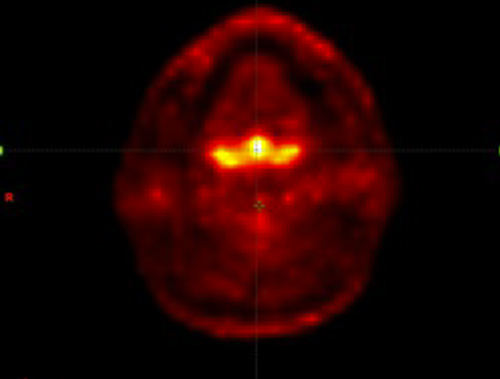
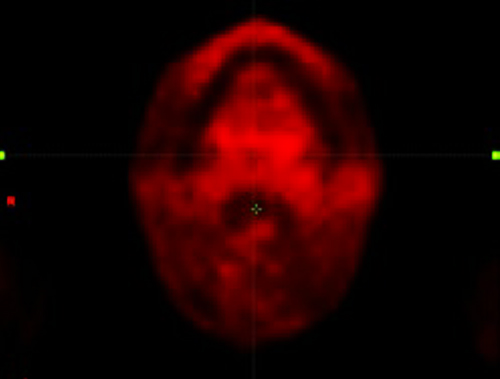
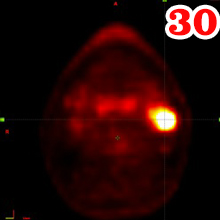
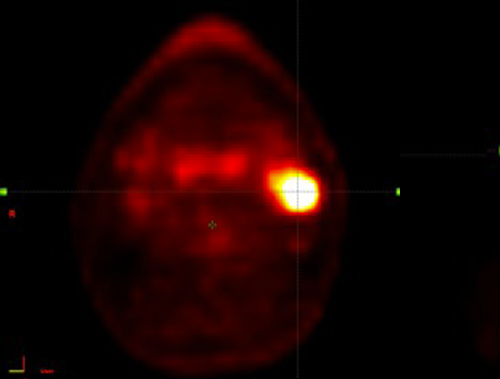
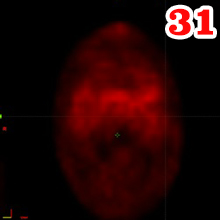
Comparison of Pre & Post Treatment PET-CT. Both PET-CT images were fused with Planning CT.
28: Pre-treatment PET-CT showing primary disease in the Base of Tongue.
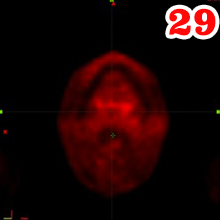
Fig 29: Post- treatment PET-CT showing no residual disease at the same site.
Fig 30: Pre-treatment PET-CT showing nodal disease at the left level II of neck.
Fig 31: Post- treatment PET-CT showing no residual disease at the same site.
Mr. X Y Z completed treatment successfully. Due to the location of the primary tumor in the base of tongue, a critical area involved in the process of swallowing, he was advised prophylactic nasogastric tube placement in the 4th week of treatment to maintain adequate nutrition. This was removed 2 weeks after completion of treatment.
Nearing the end of treatment, the patient also developed confluent mucositis in the oral cavity, which was managed with pain medications (Oral & IV) & local anesthetic gargles, for which he was admitted for a duration of 5 days.
3 months after completion of treatment, he was reviewed with a PET-CT which showed Complete Response & no evidence of residual or recurrent disease. The post treatment PET- CT was imported into the treatment planning system to verify the findings reported.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}