ContactUs
Rajiv Gandhi Cancer Institute and Research Centre
New Delhi - 110085
Rajiv Gandhi Cancer Institute and Research Centre
New Delhi - 110085
Mrs B, a 52 years old lady presented to us with complaints of persistently worsening cough for the last 3 & 1/2 months, generalized weakness associated with decreased appetite for the last 2 months & 2-3 episodes of blood-tinged sputum produced on vigorous coughing in the last 1 week. She also related that the quantity of blood was more on the last episode which occurred 2 days ago.
Image guided radiotherapy, four dimensional imaging and Linear Accelerator (capable of capturing internal organ motion) are all part of technological innovations which empowers radiation oncologists to treat most challenging scenarios in oncology.
The patient was apparently well approximately 3 & 1/2 months back when she first noticed the cough, which was initially controlled on over-the-counter cough suppressants. However, upon stopping the cough suppressants, the cough returned and persisted. She subsequently presented to a GP who ordered a Chest X-Ray and the report was suggestive of a chest infection. She was prescribed antibiotics and was asked to return after 2 weeks.
However, the patient subsequently did not return to the GP due to some personal problems. Her cough persisted & she also started feeling fatigued all the time. She attributed this to decreased appetite.
A week ago, the patient noticed a few streaks of blood after an episode of vigorous coughing. She returned to the GP and a contrast enhanced CT (CECT) scan of the chest was done. She was then referred to us for further evaluation and management.
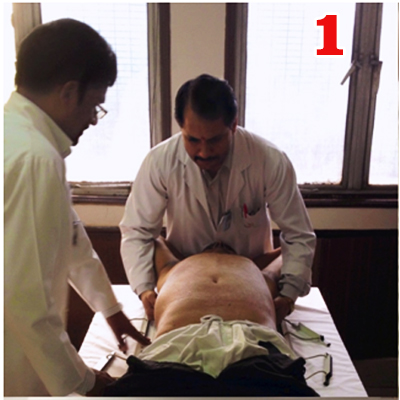
No significant past medical or surgical history. Upon clinical examination, patient appeared of Average build with BMI - 26. Her vitals were normal. Her Karnofsky Performance Score was 90. No pallor/ icterus/ cyanosis/ clubbing/Lymphadenopathy/ pedal edema/ elevated JVP was noted.
Her physical examination was normal. Her CECT revealed a 4cm irregular contrast enhancing lesion in the left lung, which was encasing the left branch of the pulmonary artery. A CT guided FNAC from the lesion revealed Non-Small Cell Carcinoma. A PET-CT was done to evaluate presence of additional metastatic spread, which was negative. Final diagnosis - Non-Small Cell Carcinoma of the left Lung.
The Radiotherapy process starts with the Radiation Oncologist discussing the need for radiotherapy with the patient & family under the following 5 headings, viz. Indication, Goal, Volume, Technique& Dose/ Time.
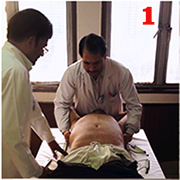
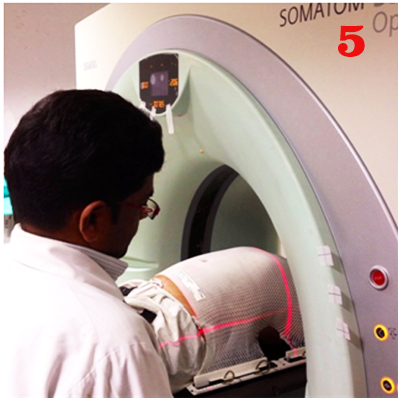
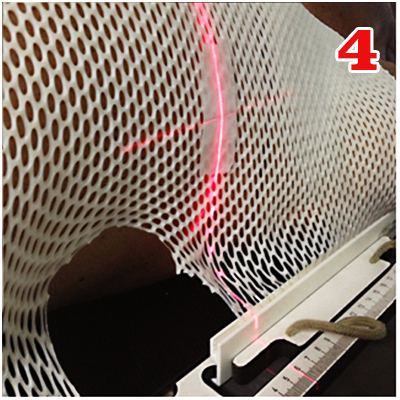
The simulation process consists of positioning the patient, creating a custom immobilization cast (to maintain the same position over all treatment days) & undergoing a high resolution contrast enhanced planning-CT scan.
Due to the mobile nature of the lung & the location of the tumor, the patient underwent several additional scans through a smaller region of the chest, harboring the tumor. These were done in different phases of the breathing cycle to study the effects of lung movement on tumor position, as well as any deformation of the tumor shape.
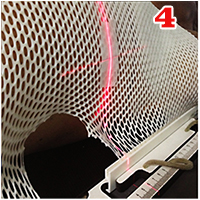
Simulation (continued).Fig 5: The laser guidance system places a reference point which aids in setting up the patient for treatment and also aids in treatment planning. Fig 6: The patient then undergoes a Contrast enhanced CT scan which is then used for treatment planning, after being imported into the Treatment planning system.
Treatment planning starts with a thorough evaluation of the planning CT by the radiation oncologist. Evaluation is focussed on correlating findings on clinical examination with radiological findings on the planning-CT. The aim is to ultimately create an accurate 3-Dimensional model of the patient, delineating the areas which are to be irradiated& important areas to be protected.
The medical physicist then analyzes this data and arranges multiple treatment beams with varying intensities to create a treatment plan. The treatment plan is then evaluated by the radiation oncologist & approved for implementation.
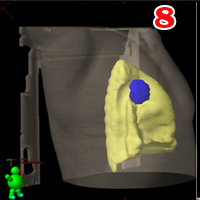
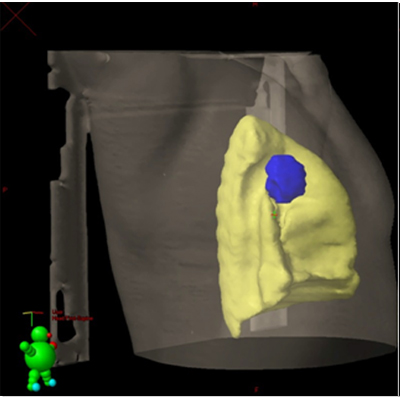
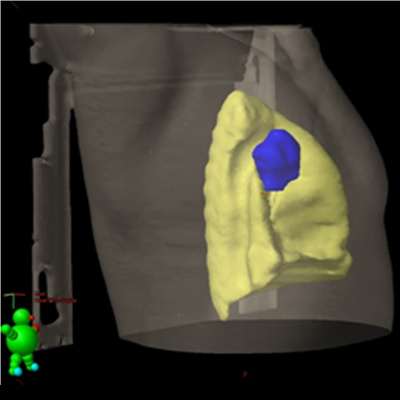
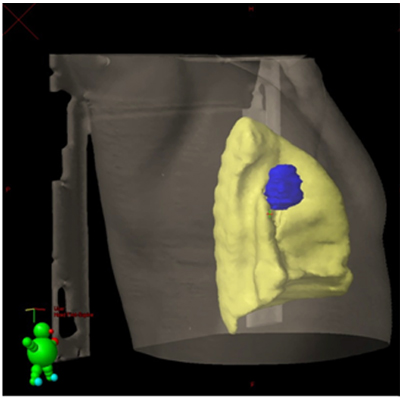
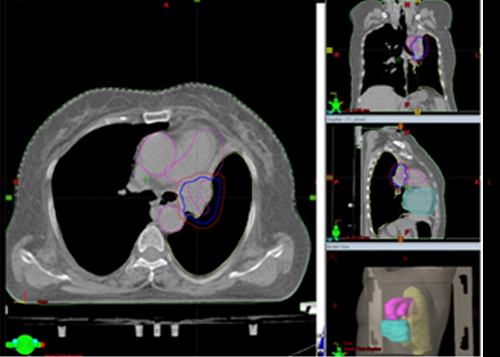
Treatment planning. Gross Tumor Volume (GTV)(shown in Blue) - The visible tumor is contoured on the Contrast enhanced CT scan in various phases of respiration. Fig 7: GTV in Inspiratory phase. Fig 8: GTV in Expiratory phase. The normal left lung is shown in yellow.
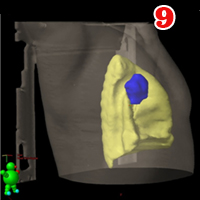
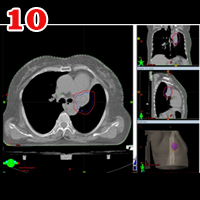
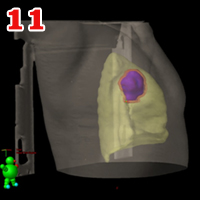
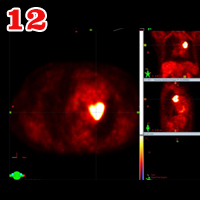
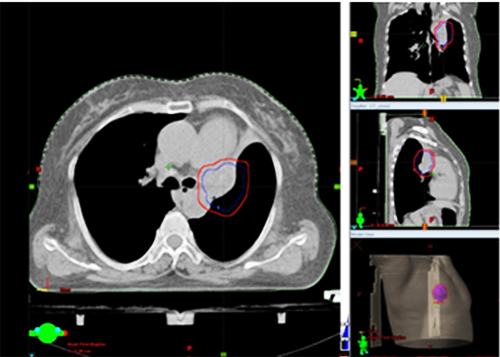
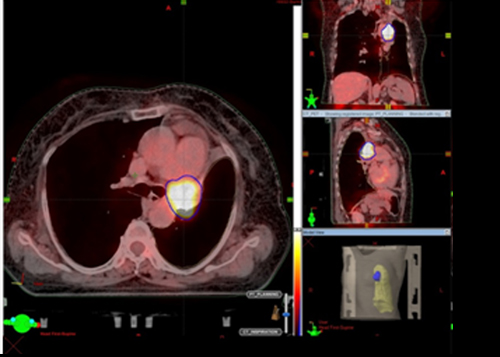
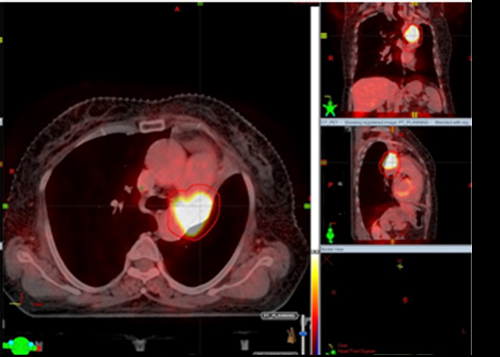
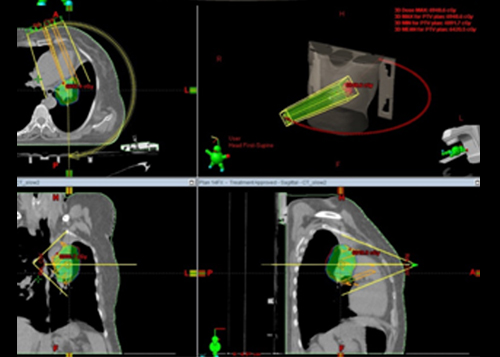
Treatment planning (continued).Fig 9: The final GTV is created after combining the GTV's created in figures 7 & 8, as well as the PET-CT (Fig 12). Figs 10 & 11:The GTV is given a 5 mm margin, the PTV (Planning Target Volume)(Red) - This is to account for daily variations which may arise.
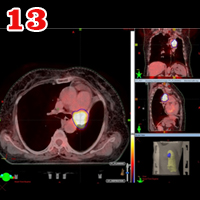
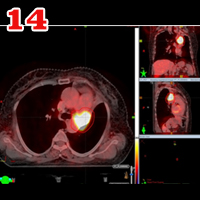
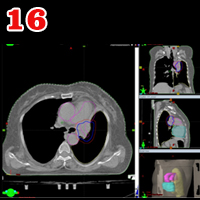
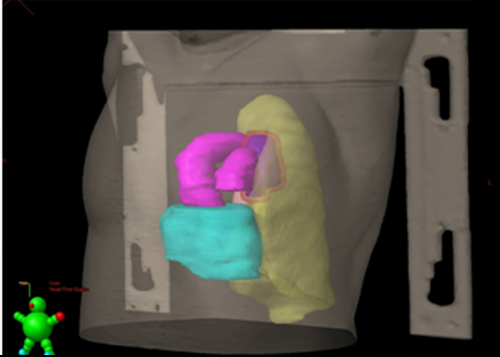
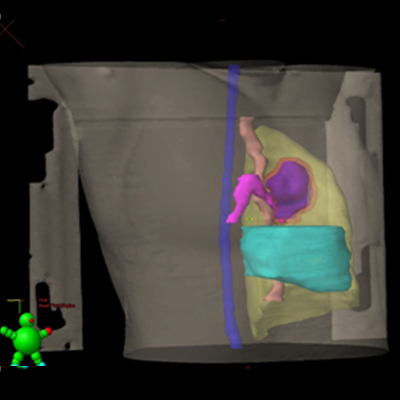
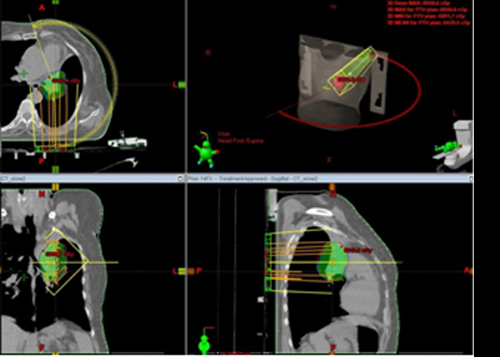
Fig13 & 14: The final GTV & PTV is compared with the PET-CT to ensure adequate coverage. Figs 15 & 16: The close proximity of critical structures to the PTV is highlighted in this 3D Model of the patient. Note the great vessels (Aorta, Pulmonary artery - in pink) & the heart (Light blue). Note the tumor encasing the pulmonary artery in fig 16 (Arrow)
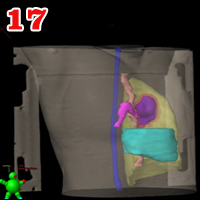
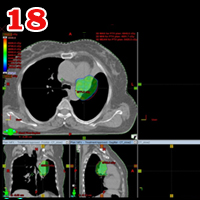
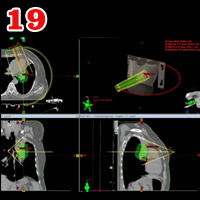
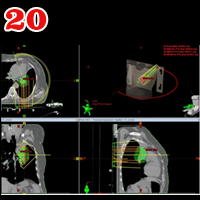
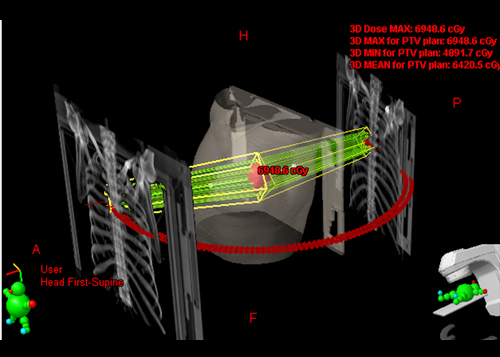
Fig 17: Additional critical structures. Tracheo-bronchial tree (pink), esophagus (brown), spinal cord (blue). Fig 18: Dose color wash around the PTV. Fig 19: The radiation beam moves around the patient, in a clockwise arc, modulating the intensity of the beam as it rotates. Fig 20: The counterclockwise radiation beam.
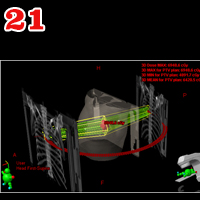
Fig 21: The combined radiation arcs provide the required level of accuracy and speed to complete treatment in minimal time.
Once the plan is ready, it is ready to be implemented on the patient, usually after an interval of 2-3 days after undergoing simulation.
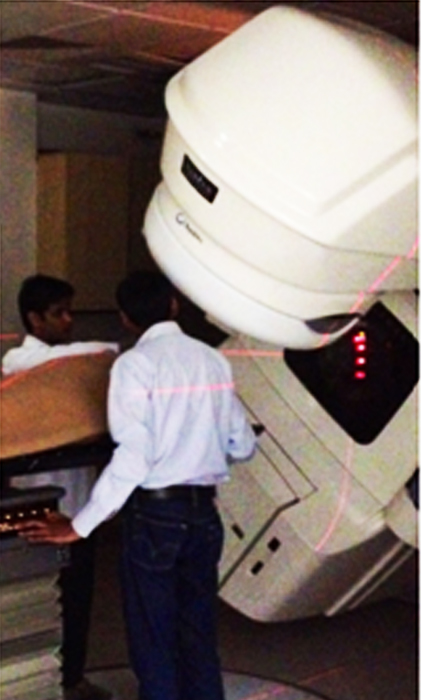
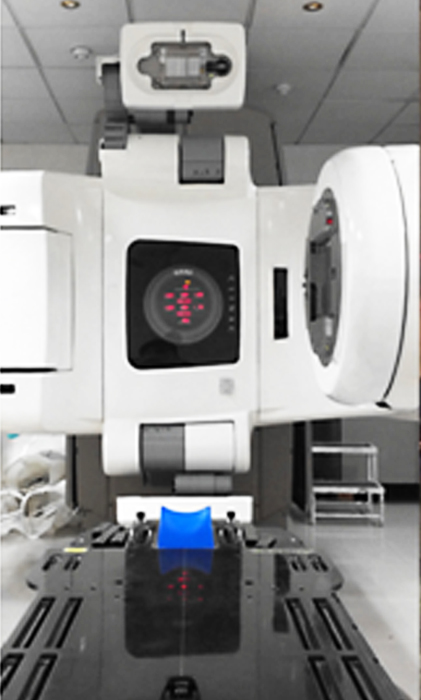
The process of plan implementation is a technically intensive process, as the data from the treatment planning system is transferred to the treatment machine (In this case, Varian Clinac 2100c RapidArc with a Cone beam CT [On Board Imager]) Implementation consists of setup & treatment delivery in the same position as simulation. The principles of setup remain the same as that of simulation. The laser guidance system on the machine & on the CT Simulator (at the time of simulation) help in further verifying that the patient is accurately set up. Prior to treatment delivery, verification CT scan is done on the treatment Prior to treatment delivery, verification CT scan is done on the treatment machine with the On Board Imager. The verification CT is then matched to the Planning CT to further increase the accuracy of treatment delivery.
Once the plan is accurately matched, the first treatment fraction is delivered. Subsequently, when the patient arrives for further fractions, the time required to deliver the treatment is reduced significantly.
During the course of treatment, patients are reviewed weekly by the radiation oncologist & blood tests done.
Precautions concerning skin care & nutrition which the patient needs to follow are also explained to the patient.
Implementation. Fig 22: Varian Clinac 2100c RapidArc with Cone Beam CT (On Board Imager). Fig 23: Patient's position is confirmed using the laser guidance system, following which patient is ready for receiving the first fraction of Radiotherapy.
The patient completed treatment successfully and with no side effects during the full course of treatment. He was advised to follow up after 6 weeks.
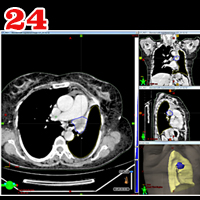
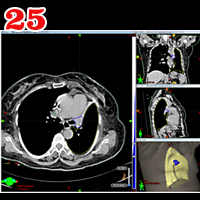
He underwent a CECT Thorax which revealed 60% reduction in size. The patient also related reduction in frequency of cough & no fresh episode of hemoptysis since completion of treatment (Figures 24 & 25).
Comparison of Pre & Post Treatment CT scans Fig 24: Pretreatment GTV (Blue). Volume of GTV - 25.8 cm3. Fig 25: Post treatment GTV at 6 weeks (Blue). Volume of GTV - 9.7 cm3.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}